Endotracheal tube in the Pharynx for Ventilating Difficult Airways
Sep 11, 2025The most feared airway scenario is Can't Intubate, Can't Oxygenate (CICO).
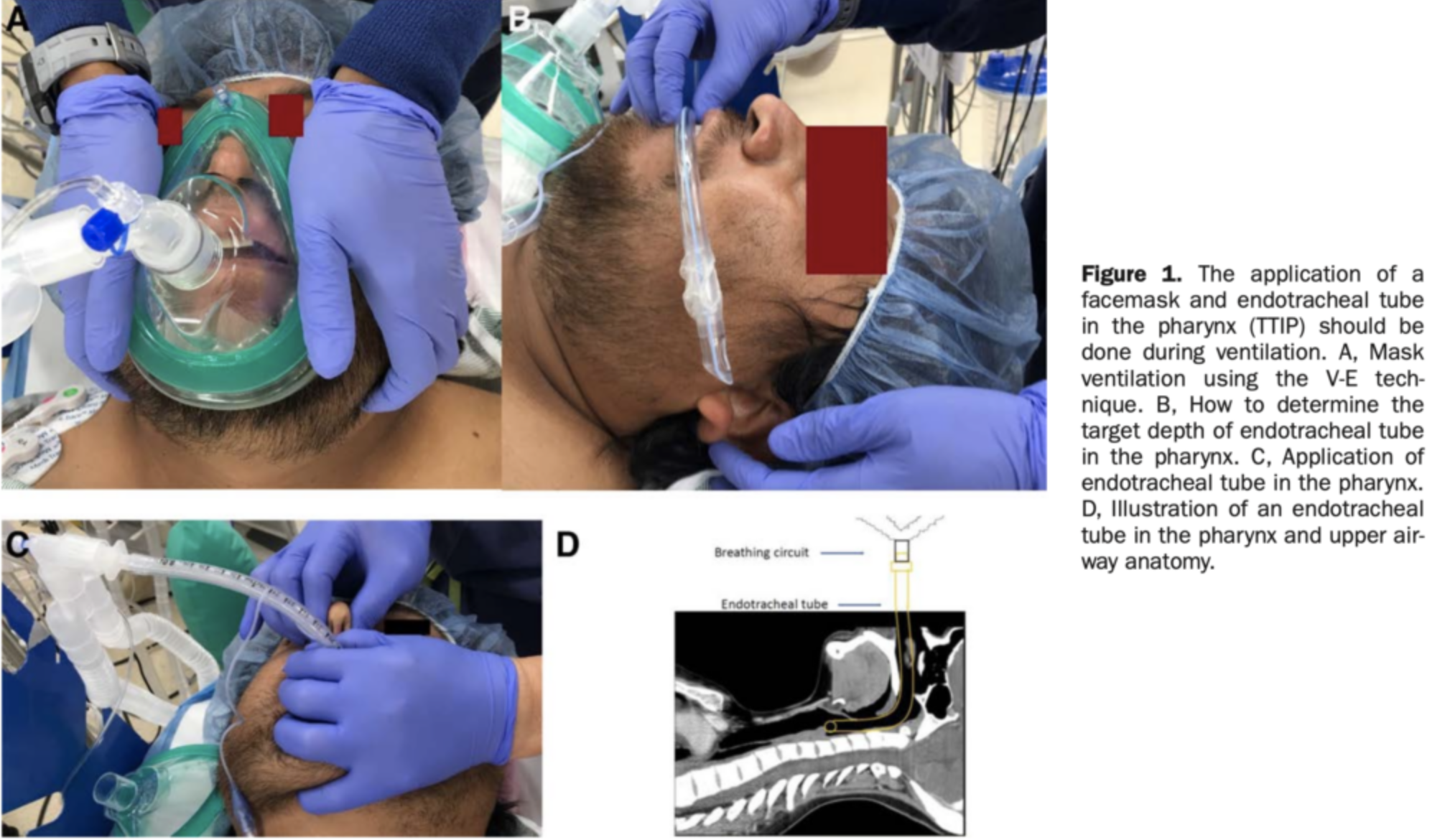
This study looked at a potential alternative to the rescue procedure of 'front of neck access' ie the surgical airway. The placement of an endotracheal tube in the pharynx was used as a rescue procedure to failed mask ventilation.
The Study
Markham T. et al. Effectiveness of Ventilation via an Endotracheal Tube in Pharynx Versus a Facemask in Patients With Potentially Difficult Airway: A Randomised, Crossover, and Blind Trial. Anesth Analg. 2025 Feb 1;140(2):280-289.PMID: 39705182
What They Did
This is an anaesthetics study, conducted in the main operating rooms of one hospital in the US.
Airway obstruction in the unconscious patient tends to occur in the upper airwayand involves tongue, soft palate and pharyngeal muscle paralysis. Can an endotracheal tube in the pharynx bypass these structures and overcome any obstruction?
In this study, they tested the hypothesis that an endotracheal tube in the pharynx is as effective as mask ventilation in the unconscious patient.
N=147
Primary Outcome
Success rates of ventilation using an endotracheal tube in the pharynx(TTIP) in patients with a potentially difficult airway. A successful ventilation was defined as a CO2 waveform being observed on capnography.
A Potentially difficult airway was defined as:
- At least 1 risk factor of a difficult airway,
- BMI >30kg/m2, and/or
- Mallampati class III or IV.
Patients were excluded if:
- They had acute or chronic respiratory disorders such as COPD and Asthma.
- They were requiring rapid sequence induction
- They required awake intubation
- They were pregnant
- There was a contraindication to a mask.
The Procedure:
- Preoxygenation via plastic facemask; flow rate of 10L minute−1 of 100% oxygen.
- When expired oxygen concentration ≥80%, induction was commenced with IV fentanyl (1–2 µg/kg), propofol (1–2 mg/ kg), and rocuronium (0.6 mg/kg).
- At apnea, ventilation was delivered by one of two methods:
- BVM with two handed technique or
- Endotracheal tube blindly inserted (into the pharynx). The depth being equal to the curvature length from the ear canal to the upper incisor
N = 136 patients: 71 in the tube first sequence and 65 in the Mask first sequence. This was a crossover trial.
What They Found
The overall success rates were:
- 93.4% (127/136) with TTIP ventilation
- 84.6% (115/136) with mask ventilation
The success rates in terms of sequence used were:
- TTIP first, 7 (9.9%) out of 71 patients failed. Of these 7 patients, 6 (85.7%) were successfully rescued with mask ventilation.
- In mask first, 13 (20.0%) out of 65 patients failed. All 13 patients (100%) were rescued with TTIP ventilation.
- One patient failed both forms of ventilation and was successfully intubated.
Other measure included peak inspiratory pressures, of which there was no difference, the ETCO2 difference between the two methods was different (TTIP and BVM ventilation (2.1mm Hg).
The key finding that the TTIP can act as a rescue device for a failed mask, is a key finding. The theory behind this, is that with a mask, the ventilation is downward and may even worsen obstruction. In comparison, the TTIP, usually bypasses the obstruction. Further, the positive pressure may keep the airway open and is usually an upward pressure.
The Verdict
We need to remember that this is an anaesthetics, theatre study, not an emergency department study. There are some very important points to take from this.
The endotracheal tube in the pharynx is not the only rescue procedure available. Airway adjuncts were not used. In my view this is the greatest weakness of this study. It would have been appropriate to compare mask with an oral airway in place.
Why not just insert a supra-glottic airway(SGA)? SGA's have a <70% success rate in rescuing CICO in the perioperative setting. Why not use a video laryngoscope?
Other concerns are that the landmarks for the depth of the endotracheal tube taken as the tube length from the ear canal to the upper incisor were arbitrarily chosen. Having said that, they appeared to work.
There are areas of obvious bias, such as practitioners not randomly being randomly assigned, not blinded to the intervention.
Will it change my practice? Not change it it, but it gives me one more tool I can use, but probably won't. The key in any technique we use is not to delay the definitive surgical airway. But maybe, just maybe, this buys time.
Join Our Free email updates
Get breaking news articles right in your inbox. Never miss a new article.
We hate SPAM. We will never sell your information, for any reason.