D-dimer to rule out Acute Aortic Syndrome
Aug 07, 2024Patients with acute aortic syndrome, may be very difficult to diagnose. Patients who present with textbook ripping severe chest pain and accompanying focal neurology and have findings of a pulse deficit and blood pressure difference in the upper limbs as well as a new aortic incompetence murmur and a new pericardial effusion on point of care ultrasound, are straightforward. Many cases however are not so textbook and patient can present with no chest pain, but symptoms of malperfusion following a dissection, presenting challenge to making the diagnosis. (20 minutes read)
In this review the question they wanted to answer was, can the D-dimer (DD) with the Aortic Dissection Detection Risk Score (ADD-RS)(1), in low risk patients, be used to rule out Acute Aortic Syndromes (AAS)? This would see its application in the same way as we use the DD with low risk patients to rule out deep venous thrombosis or pulmonary embolism.

This was a systematic review of the ADD-RS plus DD to rule out acute aortic syndromes (2). Of all studies found, 4 studies were reviewed. A total of 3804 patients were included. 675 patients had AAS.
What They Did
This was an online review of the literature.
Inclusion Criteria:
- Original research assessing integration of ADD-RS with DD to diagnose of AAS.
- Cross-sectional diagnostic studies.
- Had prospective or retrospective enrolment with AAS symptoms including chest pain, abdominal pain, back pain, syncope and perfusion deficit.
- A ADD-RS was calculated.
- A DD was measured.
- Diagnosis was confirmed or excluded with criteria including advanced imaging with CTA, transesophageal echocardiography, magnetic resonance angiography, aortography, surgery or autopsy.
- Absolute numbers of true positive (TP), true negative (TN), false positive (FP), and false negative (FN) were reported or could be determined.
Exclusion Criteria:
- The design was case–control or case series
- Conference abstracts
Two DD cut-offs were used: DD < 500ng/mL and an age adjusted DD.
The following was analysed:
- ADD-RS ≤ 1 and DD < 500 ng/mL
- ADD-RS ≤ 1 and DD < DD age-adj
- ADD-RS = 0 and DD < 500 ng/mL
- ADD-RS = 0 and DD < DD age-adj.
What They Found
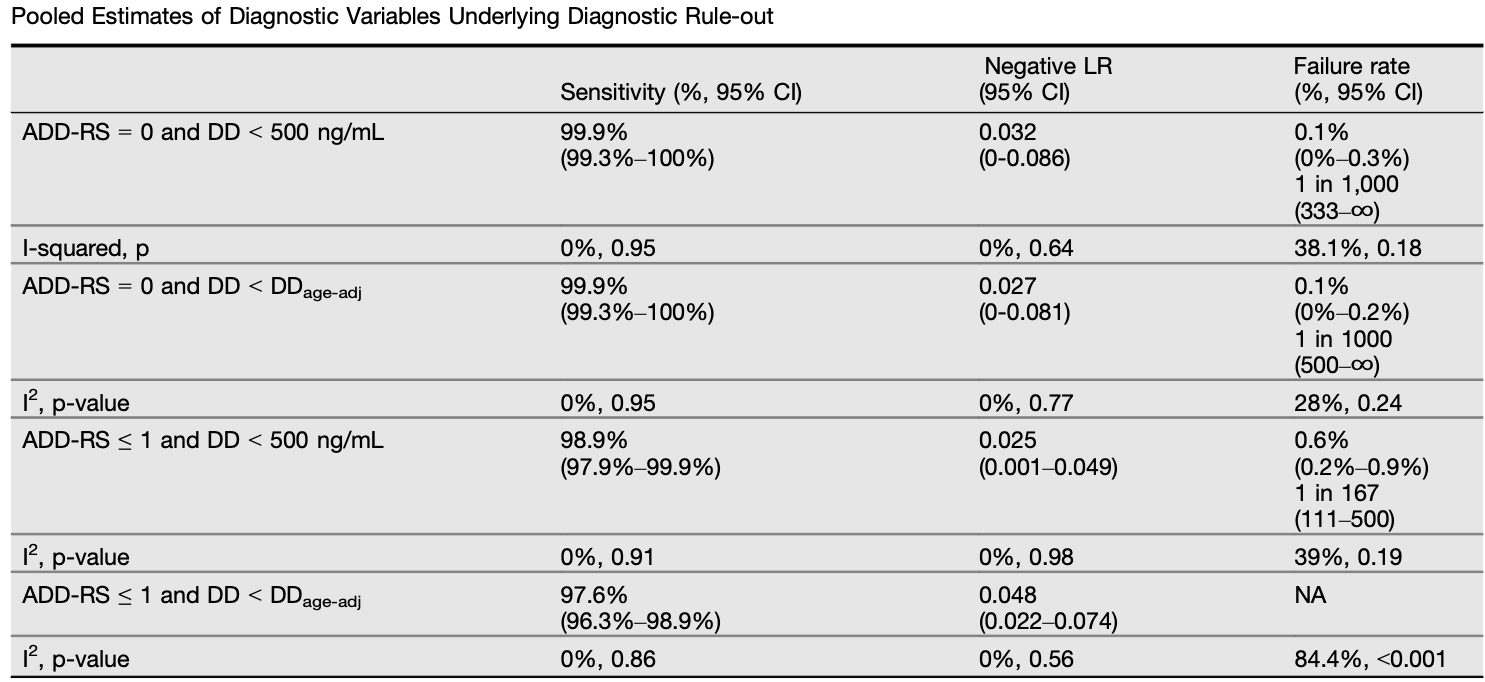
"Available studies consistently show that ADD-RS = 0 or ≤ 1 plus DD <500 ng/mL are highly sensitive diagnostic strategies and support their reliability for rule-out of AAS."
My Take on This
This study asked a specific and important question in its search for research to review: Can a low ADD-RS and 'normal' DD, be used to rule out AAS? 4 studies were included. One was a prospective multi centre study, the other three were retrospective studies. All were emergency department studies and most included patients with chest pain.
The inclusion criteria in these studies differed and a limitation is that there was no standard definition of what a patient with suspected AAS is.
We need to beware as the ASS-RS has a low specificity and has been derived from a register of AAS patients. We are not sure if using the ADD-RS provides any advantage in terms of ordering tests such as a CT angiogram.
What this means as with using the DD to rule out DVT or PE, is that we must use it on a specific population ie., the low risk population. The study does not support using an age adjusted DD at this point.
We need prospective trials to look at this. However for the low risk patient it may be something to consider. (Please review Acute Aortic Syndromes)
References
- Bima P et al. Systematic Review of Aortic Dissection Detection Risk Score Plus D-dimer for Diagnostic Rule-out of Suspected Acute Aortic Syndrome. Acad Emerg Med. 2020;27(10):1013-1027
Join Our Free email updates
Get breaking news articles right in your inbox. Never miss a new article.
We hate SPAM. We will never sell your information, for any reason.